

In any given moment we have two options; to step forward into growth or step back into safety
Abraham Maslow
Maslow described a hierarchy of needs – others have adapted the same to describe basic hygiene needs and relatedness needs that lead to self-actualisation or growth. It is peculiar to western culture that we consider the self as a single entity in contrast to Eastern cultures where the self is recognised as having several component parts. I drew on this for my MB thesis in submitted in 2005 to highlight the needs of our various selves which are really defined by context from the macro to the microenvironment. We can debate the adjectives that I used at the time but essentially the bottom two steps are Alderfer’s hygiene needs, or existence needs without which we cannot progress. They represent the transactional nature of HR (I too do not like the word Human Resources as I do not believe people should be considered a resource). If the pay and conditions are not right most people would walk. In clinical terms, I would include out of hours provision of food and rest and recuperation facilities. At the team level ‘psychological safety’ is paramount - the RCSEd ‘#letsremoveit’ campaign has highlighted this imperative.
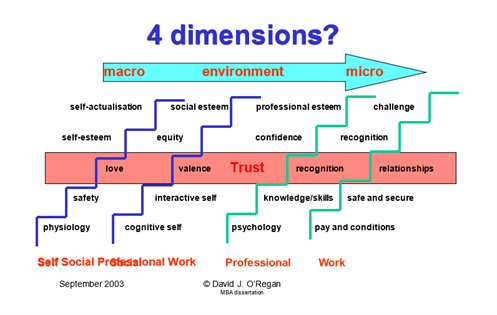
The middle or third step - relatedness needs - revolves around trust and the building of relationships. I consider this the ‘water mark’ as in the phrase holding one’s head above water’. This step encompasses social and external esteem, and this is built on the relationship with significant others; family or spouse for the self, valence for the social self and recognition as being part of the team for the professional self. The latter is the foundations of legitimate peripheral participation i.e. you are welcomed as part of the team and your opinions count. Are we affording this as a ‘right’ to trainees or is it still considered a ‘rite’ of passage? It is getting better, but we have a lot to learn.
Relatedness is founded on trust and the more relatedness needs are satisfied; the more growth needs will be desired – this is called nurturing. Our involvement as trainers in trainee development and assisting in their own self actualisation, is pastoral
In my previous blog I lamented the decision to change the new means of assessment of trainee from ‘EPA’ (Entrustable Professional Activity) to a ‘CIP’ (Competence in Practice). The UK in their wisdom yet again demonstrates their determination to go it alone by ignoring well researched and published data from around the globe. I first talked about ‘Trust’ in a blog from July 2020.
The training system present designed to assess COMPETENCY and CONSISTENCY with a combination of formative and summative assessment that converts into a numerical score to determine progression. Does the trainee get their head above water? The process itself reinforces the tick box ‘transactional’ approach to learning and a satisfactory will do. It is very unilateral and requires the trainee to fulfil those conditions to earn the trust of the trainer and the system. The fulfilment of this transaction condescends the right of passage to the next step.
Too often we hear from trainees that they must spend a period earning the trust of the trainer before they are permitted to do anything at all. This may take a few weeks but, in some cases, may take many months. I reflect on the comment made by Gillian Hardman on a recent Faculty of Surgical Trainers webinar – she has had eleven ‘first days at school’ and has had to work to earn the trust of the trainer. If these weeks, if not months, are added up over a training program, it becomes obvious that the trainee must ‘earn’ trust over a significant part of their training. The mere fact that they have been through rigorous selection and assessment as well as invested significantly financially over time in their professional development, does not appear to come into consideration. This is fundamentally wrong at every level, not least the fact we do not treat our trainees as adulty learners. This is an opinion shared among the FST executive.
So, what is trust – well at the present it is a term of convenience. It is a flexible, if not a warped term, that justifies a service that is largely dependent on the trainees. Consultants and the system trust the trainee to deliver a service and occupy the shop floor as the first point of contact for almost everything the NHS delivers. The most unpredictable element of any job is out of hours. We have all been moved by the story of the trainee overwhelmed by systemic issues, covering many patients, and then prosecuted by the system for doing her very best. What of the consultant in charge – they absconded and ducked their responsibility to support the trainee. I am happy to call it out as it was – shameful!
At the very least the training consultant must have the back of the trainee and the trainee must be comfortable to call the consultant, no matter what – psychological safety is paramount. Standing up for the trainee, respecting their identity and supporting their learning must be a given. Every trainee deserves respect and has potential – if you do not believe that, you do not deserve to be a trainer.
Likewise, it is the duty of the trainee to be honest and give their feedback. It is however important that they understand their limitations and recognise the areas that need attention to grow. A derailer in this relationship is lack of insight. I celebrated the first solo top end of a trainee, having stood opposite the bottom ends (term for coronary artery bypass grafts). I returned from the adjacent room and was delighted that the quiet theatre, reassuring sinus rhythm, accompanied by the satisfying beep, and calm of the anaesthetist, affirmed that all was well. But was it? I enquired of the trainee what they thought of the top ends and the reply came back, ‘you will not like them’. The trainee was closing the chest and had given protamine to reverse the heparin needed for bypass. I asked to look at the top ends and agreed that I did not like them. I suggested the trainee get some coffee and I took over. At a debriefing the following day the trainee confirmed that they would have been happy to close the chest and would have done so if I had not come in and enquired. I explained that bottom line was that we were there to serve the patient and deliver an operation that would not need further intervention for at least nineteen years – that being the number of years I had been a consultant cardiac surgeon. The biggest antagonist to trust is lack of insight and failure to recognise fallibility – the best line from a Clint Eastwood film was ‘a man has to know his limitations’.
This is the water mark – trust in the trainee and vice versa. If there is no trust, there is no chance of growing, everyone can learn. The relationship should be mutually benefiting, enabling both parties to grow. Parenting is the same, communication needs to be clear, supportive, and encouraging. We need to be honest on both sides especially if we get it wrong. Learn not blame, compassion, integrity, fallibility and humility come into the equation. It is okay not to know but it is not okay to ignore you do not know and most definitely not okay to accept you do not know.
So, the question is, do we have a system that can determine the level of trust that can that be codified into a quantum of trust that passes to the next trainer? Well, we do. It is called CIP - trainees are encouraged to fill their portfolios with CIP’s i.e. they are entrusted to carry out the procedure by themselves. Experience is a volume of competency, and it is heartening to see that Professor Tim Briggs of GIRFT is proposing high-volume low-cost centres where a single consultant will oversee several trainees building their experience of registered CIP’s. Sorry but every time I write CIP, I think SIP ‘a martini, ‘shaken not stirred’ – the 007 beverage. CIP is in fact a license not to kill but to trust someone with another’s life.
Trust exemplified in character. It is open and honest and true to their word – the key value prized among many is integrity. Does the individual walk the talk, and seek and respect other opinions? Do they listen in the present? Are they able to walk in others’ shoes and do they show empathy? Does character respect the person and can they demonstrate compassion and empathy? This relationship now becomes transformative. Trust is no longer learned but it is generative. This demands of both the trainer and trainee as it becomes restorative and empowering. It requires effort and the commitment of both the trainer and trainee to self-develop. The relationship enters the stages of growing a self-actualisation.
These skills can be learned and practiced by both parties through respective attention, thinking, listening and compassion (ATLC). We can learn and practice be being present and attending to how we communicate. The acronym ATLC is deliberate with an emphasis on TLC – after all, we all need it!
It is really a mindset – listening to the winners of the Silver Scalpel Award, BOTA Award for the best trainer and the Silver Suture Award on the Faculty of Surgical Trainers webinar on 21 September 2021, we all can and should do it! It is our mindsets that govern how we make sense of the world and everything we experience. As trainers we have an awesome role and responsibility in this process of realising needs. We need to encourage growth by focusing on learning goals and shift our dialogue from a critic to a kind, wise friend. We need to be mindful of our thoughts and actions each day, by learning from our successes and failures so we can be agile and adapt. We need to consider more than what we just do and be able to explain the how and why. This is described by Dr Paige Williams in her book published in 2020 – Becoming Antifragile – learning to thrive through disruption, challenge, and change. A must read for all - especially trainees.
This is not just here now but it is more a thinking of the infinite game as described by Simon Sinek. This then becomes transcendental – the larva leaves the water surface as beautiful dragonfly. This is the emancipation of the individual, self-actualisation, worth and growth. It is not just what we say and do as trainers, it is how we say it and do it that anchors role models for the future surgeon.
How do we capture this in the Speciality Training Review, ARCP? Well the MCR process will go a long way to alleviating personal biases and heuristics and trainers will be held to account be peers. This is all very good but how are we going to codify these attributes of a trainer? Framework 7 of the FST standards outline some of the attributes but I believe they can and should go further to include the aforementioned. I am not suggesting that we have a trust rating score, but I do believe we need to recognise and accredit those trainers that do this day in and day out and may not necessarily have and may not be able to demonstrate any academic educational qualifications or experience. What is more important is that they are demonstrating all the skills and attributes of a good trainer as recognised by the trainees.
In true customer service feedback, it is recommended that we only count 5/5 scores. The difference between 5/5 and 4/5 on a Likert score of satisfaction is the ‘wow’ factor. The only company in the world that works and depends on 5/5 is Disney, because if they did not deliver 5/5 consistently, people would not go back or talk about them. Disney depends on 5/5 now and for future audiences. The question is can we build a system that recognises and supports 5/5 trainers? I believe we can, and all trainers should be encouraged to use the ISCP website. I am encouraging the FST to recognise the 5/5 trainer, that is what the Faculty is all about.
A few questions remain
Send your thoughts to fst@rcsed.ac.uk
Select a year and month from the headings below to view blog posts from that month.
Due to essential systems maintenance and upgrades there will be interruptions to some on-line services on Saturday 19th of August.
We apologise for any inconvenience caused.
×